WHAT HAPPENS IN THE BODY
The anatomy of injury
What Happens When you Get Hurt?
Injuries can feel confusing and sudden — but when you break it down, your body is actually doing its job trying to protect and repair you.
There are two main types of injuries student-athletes face:
Acute Injuries: These happen in a single moment. Think a hard landing, a twist, a fall, or contact that causes immediate pain — like a rolled ankle, a broken bone, or an ACL tear.
Overuse Injuries: These build up over time. They’re caused by repetitive stress or loading without enough rest. Common ones include shin splints, tendinitis, or stress fractures.
WHAT’S HAPPENING INSIDE YOUR BODY DURING INJURY?
Tissue Damage: Muscles, tendons, ligaments, cartilage, or bone can tear, strain, or crack.
Inflammation Begins: Your body sends blood and healing cells to the area — causing swelling, redness, heat, and stiffness.
Pain Signals Fire: Nerves in the injured area send pain messages to your brain to tell you to back off and protect it.
Muscles Around the Area React: They might tighten or “guard” to protect the injury, but that can also limit movement and make you feel unstable.
WHY YOU FEEL WHAT YOU FEEL…
Swelling? That’s fluid and cells rushing in to help heal.
Stiffness? Your joints are trying to stay safe and avoid more damage.
Pain with movement? That’s your brain flagging to your body “I’m not ready yet.”
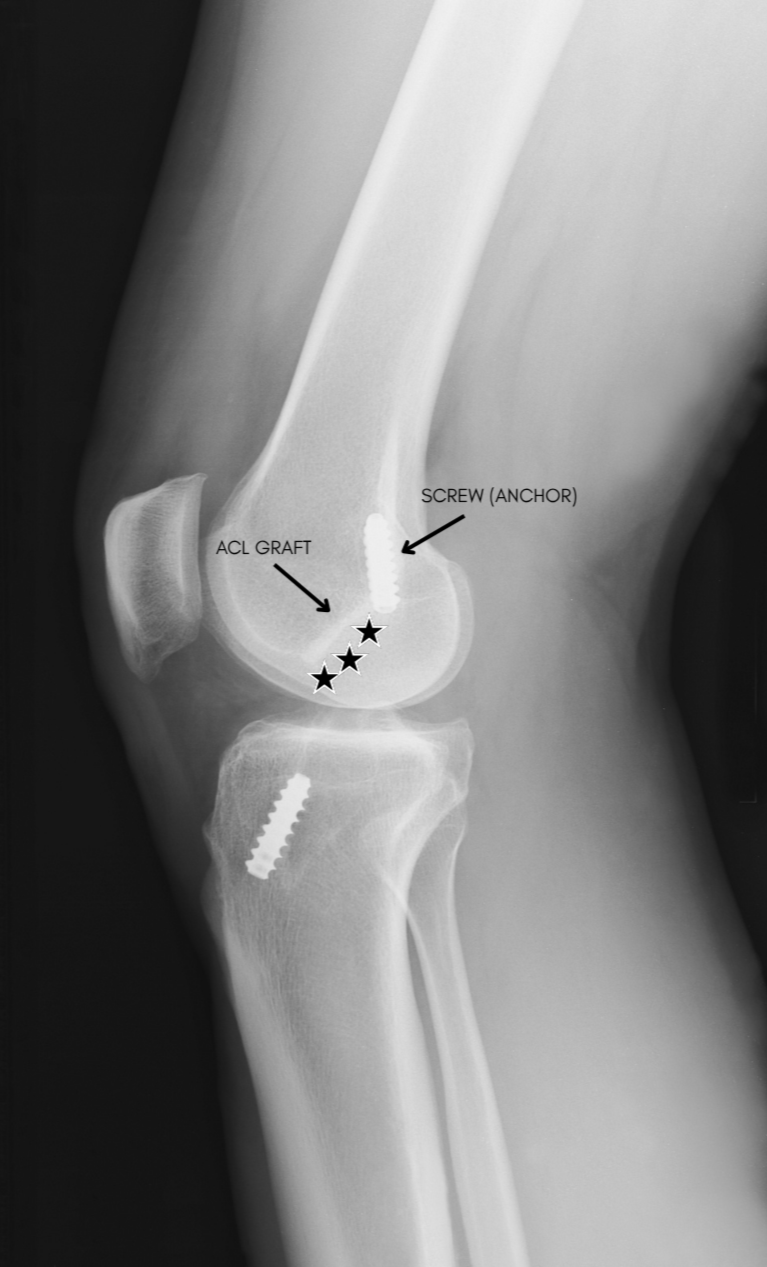
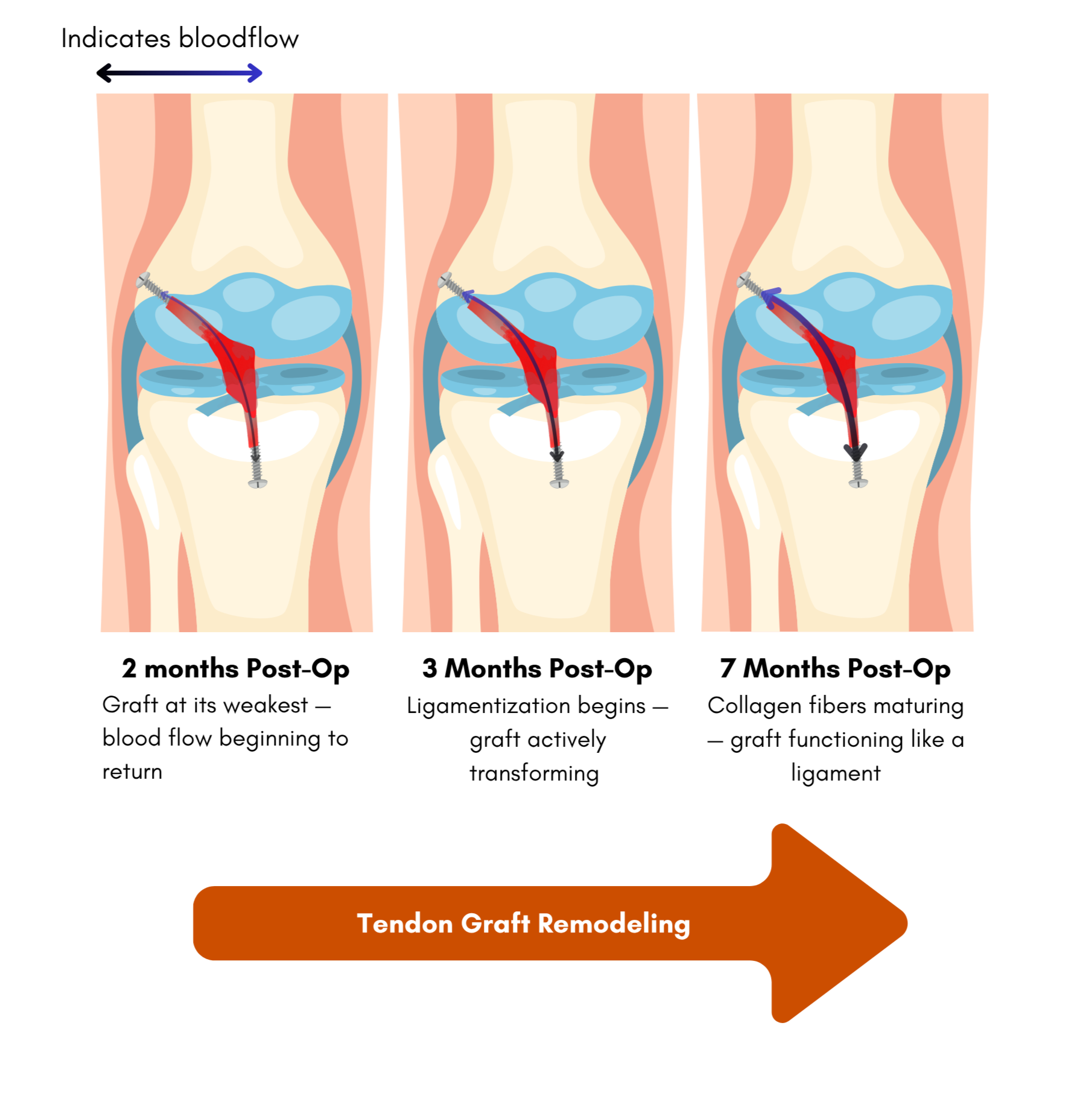
FUN FACT — YOUR ACL GRACT HAS TO BECOME A LIGAMENT
When you have ACL reconstruction, your surgeon uses a tendon to replace the torn ligament — but that tendon isn't immediately a ligament. It goes through a process called ligamentization, where over 12-24 months it gradually remodels itself to function like a native ACL. During this process, the graft is actually at its weakest around 6-8 weeks post-surgery — right when most athletes start feeling better and wanting to push harder.
On top of that, your brain has to relearn how to communicate with the new tissue entirely. The nerve receptors that send signals between your knee and your brain are disrupted after injury, which is why balance, reaction time, and proprioception all take time to rebuild. Strength alone isn't enough — your nervous system has to rewire itself too.
Injuries By Type
Understanding what type of injury you have is the first step toward healing. Each injury acts differently in the body — and knowing what you’re dealing with can help you ask smarter questions, follow the right rehab, and avoid doing things that could make it worse.
Ligament Injuries
What are they? Ligaments connect bone to bone. Injuries happen when joints are pushed too far — like during a twist, collision, or awkward landing.
Examples: ACL, MCL, LCL (knee); UCL (elbow)
What they feel like: A pop, swelling, joint instability, or the feeling that something gave out.
Common in: Sports that involve cutting, jumping, or pivoting (e.g., soccer, basketball, wrestling)
Tendon Injuries
What are they? Tendons attach muscles to bones. Repetitive motion or sudden overload can lead to inflammation (tendinitis), degeneration (tendinosis), or even a tear.
Examples: Achilles tendon, patellar tendon (jumper’s knee), rotator cuff (shoulder)
What they feel like: Achy pain during movement, weakness, stiffness, or pain in the morning.
Common in: Running, volleyball, tennis, baseball, and throwing sports
Muscle Injuries
What are they? Muscle strains happen when fibers are overstretched or torn. Contusions are deep bruises from impact.
Examples: Hamstring pull, quad bruise, calf tear
What they feel like: Sharp pain, tightness, swelling, bruising, or weakness.
Grading:
Grade I: Mild pull, little to no loss of strength or movement.
Grade II: Partial tear with moderate pain and some functional loss.
Grade III: Full tear with significant weakness, pain, and swelling.
Bone & Joint Injuries
Fractures: Breaks or cracks in the bone — can be sudden (acute) or develop over time (stress fracture). Expect pain, swelling, bruising, and trouble bearing weight.
Dislocations/Subluxations: When a bone pops out of its joint fully (dislocation) or partially (subluxation). Common in the shoulder, kneecap, or fingers.
Cartilage Damage: Cartilage cushions your joints — when it tears (like a meniscus in the knee or labrum in the shoulder), you might feel catching, locking, clicking, or instability.
Why this Matters:
Each injury type needs a recovery plan. Rehab for a ligament tear isn’t the same as a muscle strain. Knowing what you’re healing from helps you stick to the right path and avoid setbacks.
Inside the Injury: A Student-Athlete’s Guide to Healing
This page was built from real experience — my own injury journey and the insights I gained from the people who helped me through it. The information here comes from trusted research studies, conversations with my athletic trainer, guidance from my surgeon Dr. Westerman, and in-depth discussions with Doug, one of the rehab professionals I worked with directly.
It’s a combination of science, lived experience, and everything I wish I’d known earlier.
Injuries suck. They slow you down, shake your confidence, and sometimes make you feel like a stranger in your own body. But the truth is, injury is part of the athlete experience — and the more you understand what’s happening, the more power you have to take your recovery into your own hands.
This page isn’t full of medical jargon. It’s for you — the student-athlete — who wants to know what’s going on inside your body, how to get back to your sport safely, and how to stay strong mentally and physically along the way.
Whether you’re currently hurt, helping a teammate through it, or just want to be ready for anything, this guide is your starting point.
Why This Page Exists: You’re an athlete. When your body takes a hit — whether it's a twist, pop, tear, or strain — you deserve to understand what’s happening and how to bounce back smarter. This page breaks it down in your language, so you can take charge of your recovery.
Disclaimer: This page is for educational purposes only and is based on personal experience, expert conversations, and trusted research. It’s not medical advice. Every injury is unique, and recovery should be guided by a licensed healthcare provider. Always consult with your athletic trainer, doctor, or physical therapist before starting or changing any treatment plan.
Take your knowledge further…
— WATCH & LEARN: UNDERSTANDING INJURY
These YouTube videos break it down in athlete-friendly language:
How to Recovery from an ACL Tear? | Knee Surgeon and Physio Explained
This video breaks down everything you need to know about ACL tears — whether you’re recovering yourself or helping a teammate through it. You’ll learn:
How to recognize an ACL tear from a knee surgeon’s perspective
Rehab tips and timelines from a physiotherapist
The long-term impact of an ACL injury if not managed properly
Prevention exercises, including plyometrics, to reduce future risk
Packed with expert insights and practical advice, this video is a solid resource for student-athletes navigating the ACL recovery journey.
Slips, Trips, and Life After Injury — with Dr. David Neuman (TEDx)
In this talk, orthopedic surgeon Dr. David Neuman explains how simple injuries — like slips, trips, or falls — can have long-lasting effects if not managed well. He offers practical advice on how to respond to acute musculoskeletal trauma and shares strategies to support recovery using physical therapy and smart home exercises.
With years of experience in sports medicine and arthroscopic surgery, Dr. Neuman emphasizes the importance of early movement, strength, and fitness in healing. This video is ideal for student-athletes looking to better understand injury recovery and reduce their risk of long-term complications.
Questions to Ask Your Surgeon (and Write Down the Answers):
About the injury itself:
What exactly was damaged in my knee/ankle/shoulder?
Will this injury fully heal, or will I always have to manage it?
About the surgery:
What graft did you use and why?
Were there any extra procedures (like LET or meniscus repair)?
About recovery:
What’s the estimated timeline before I can run, train, or compete?
What signs should I look for that say I’m progressing well (or not)?
Are there any risks of re-tear I should be aware of?
About return to sport:
What mental signs do you look for to say an athlete is truly ready?
How can I reduce my chances of getting hurt again?
READ: Injury Glossary for Student-Athletes →
Injuries come with a lot of confusing terms. This glossary breaks down the most common anatomy and injury words — so you can understand your body, ask better questions, and feel more in control of your recovery.

What’s a graft and why should I care?
If you tear a major ligament — like your ACL — you might need surgery to rebuild it. That’s where a graft comes in. A graft is a piece of tissue used to replace the damaged ligament so your knee (or other joint) can become strong and stable again.
But here’s the part no one really talks about until you’re sitting in front of the surgeon:
You (and your doctor) usually have a choice in what kind of graft to use. Your surgeon will help you make the right call based on your age, sport, activity level, and anatomy.
So What Are The Options?
There are two main categories or types of grafts:
I. AUTOGRAFTS (FROM YOUR OWN BODY)
Patellar Tendon (BTB)
Taken from the middle third of your patellar tendon (below your kneecap)
Strong and reliable
Caution: Can cause kneecap pain, especially when kneeling (Read →)
Hamstring Tendon
Comes from tendons in the back of your thigh
Less front-knee pain, smaller incision
Caution: Tends to have more laxity and has slightly higher failure rates in younger athletes (Read →)
Quadriceps Tendon
Comes from the top of your thigh, sometimes with a bone plug
Thick, strong graft with less pain during daily movement
Caution: Newer option with less long-term data; may cause some quad weakness (Read →)
Learn More: Orthopedic Reviews — What Are the Graft Options for ACL Reconstruction? →
II. ALLOGRAFTS (FROM A DONOR)
What are they?
Allografts are donated human tissues used by surgeons when a patient's own tissue (autograft) or animal tissue (xenograft) isn’t ideal. These tissues come from tissue banks, which handle the screening, recovery, and distribution.
Pro: Less pain post-op and no need for a second surgical site (Read →)
Caution: Takes longer to fully heal; slightly higher risk of re-tear in younger or high-level athletes (Read →)
What Are The Different Types?
Soft Tissue Allografts:such as an Achilles, tibialis anterior, or hamstring tendon from a tissue bank — used to replace the torn ligament the same way an autograft would, just using someone else's tissue.
(Donor) Bone-Patellar Tendon-Bone (BPTB) Allografts:Same structure as the BTB autograft but sourced from a donor. Provides bone plugs on each end for fixation and is sometimes used in revision surgeries or older patients.
Learn More: Allograft vs Autograft Failure Rates in Young Athletes — PMCAllograft Reconstruction Fails at Greater Rate Under 34 — PMC →
WHAT THE RESEARCH SUGGESTS
A 10-year follow-up study by Barié et al. (2020) compared BTB, QTB, and hamstring autografts and found a meaningful structural difference in how they heal. Patellar tendon and quad tendon grafts both allow for direct bone-to-bone integration at the fixation points, while hamstring grafts rely on soft tissue-to-bone healing — a process that takes longer and may be less mechanically stable in the early stages of recovery. This distinction is one reason some surgeons favor BTB or QTB grafts for high-level athletes returning to cutting and pivoting sports. Read the full study →
That same study noted that while patellar and quad tendon grafts offer strong healing properties, harvesting them carries real tradeoffs — including the risk of anterior knee pain, donor site discomfort, and in rare cases patellar tendon tear or fracture. No graft is without compromise.
KEY TAKEAWAYS FROM RESEARCH…
QTB autograft is increasingly considered a strong alternative to the traditional patellar tendon graft — particularly for athletes concerned about kneeling pain or quad recovery time
BPTB remains a reliable, well-studied choice for competitive athletes — with the tradeoff of higher anterior knee pain risk at the donor site
Hamstring grafts are widely used and cause less donor site pain, but research suggests slightly higher failure rates in younger athletes and a different healing timeline due to soft tissue-to-bone integration
WATCH THIS VIDEO → CHOOSING THE RIGHT GRAFT FOR YOU ACL SURGERY
This Stanford University video breaks down common ACL graft options —patellar tendon (BTB), hamstring tendon, quadriceps tendon valves, and allografts — highlighting the benefits and potential downsides of each. It’s a smart watch for any athlete gearing up to make informed decisions before surgery.
Why it's useful:
Straightforward comparison of graft types
Helpful visuals and explanations from experts
Great prep before meeting with your surgeon
What the Research Says
The research in this section comes directly from studies presented at a sports medicine conference hosted by Boston Children's Hospital Orthopedics and Sports Medicine in collaboration with Harvard Medical School. We've broken it down in plain language so you don't need a medical degree to understand your own recovery.
1. DOES IT MATTER WHICH GRAFT I GET?
The short answer: graft size may matter more than graft type.
Research presented at the conference found that when a hamstring graft reaches at least 9mm in diameter, there is no clinically meaningful difference in pain, function, or activity scores between the three main graft types — patellar tendon, hamstring, or quad tendon. What that means for you is that the conversation with your surgeon shouldn't just be about which graft to use — it should also include how they ensure the graft is strong and thick enough for your level of sport.
A separate 10-year follow-up study noted one structural difference worth understanding: patellar tendon and quad tendon grafts allow for direct bone-to-bone healing at the fixation points, while hamstring grafts rely on soft tissue-to-bone healing — a process that takes longer and may be less mechanically stable in the early stages. This is one reason some surgeons favor BTB or QTB grafts for high-level athletes, though outcomes across graft types are comparable when size is adequate.
2. IS THERE ANYTHING SURGEONS CAN ADD TO LOWER MY RE-TEAR RISK?
Yes — and it's worth asking your surgeon about.
Two additional procedures have shown meaningful reductions in re-tear rates when performed alongside standard ACL reconstruction:
ALL Reconstruction (Anterolateral Ligament): Adding ALL reconstruction alongside ACL surgery improves rotational stability — especially during twisting and cutting movements. A review of six clinical trials found that combined ACL + ALL reconstruction reduced re-rupture rates from 7.3% to 2.4% and improved knee stability scores significantly compared to ACL reconstruction alone.
Read the ALL reconstruction study →
LET (Lateral Extra-Articular Tenodesis) LET uses a strip of your iliotibial band to add rotational stability alongside your ACL graft. The STABILITY Study — one of the largest randomized clinical trials on this procedure — found that adding LET to a hamstring autograft reduced graft rupture rates from 11% to 4%, and overall clinical failure rates from 40% to 25%. Pain and function scores were similar between groups, meaning the added procedure didn't make recovery harder.
Note: These procedures aren't right for every athlete. Your surgeon will determine whether either is appropriate based on your specific case, anatomy, and risk factors.
3. WHEN IS IT ACTUALLY SAFE TO GO BACK?
Later than you think — and much later than you feel ready.
One of the most cited findings in ACL research is this: athletes who return to sport before 9 months post-surgery have a re-injury rate approximately 7 times higher than those who wait. What makes this finding particularly important is that passing strength tests or jump tests didn't protect athletes who returned too soon. Physical readiness benchmarks alone are not enough — time matters independently of how good you feel or how well you perform in testing.
The bottom line: feeling ready and being ready are not the same thing. Waiting until at least 9 months — and passing both physical and psychological readiness criteria — is one of the most evidence-backed things you can do to protect your knee.
Read the return-to-sport timing study →
4. WHAT IF I DON’T FEEL MENTALLY READY?
That feeling is real, it's documented, and it matters for your outcomes.
Research tracking athletes from before surgery through return to sport found that psychological readiness — measured by the ACL-RSI scale — improved over time for both male and female athletes, but female athletes consistently reported lower readiness to return at every stage of recovery. This isn't a personal weakness — it's a documented pattern that reflects the unique psychological challenges female athletes face during ACL recovery, including fear of re-injury, identity loss, and confidence rebuilding.
A separate study found that athletes with higher resilience — the ability to bounce back from setbacks — had significantly better knee function and quality of life at both one and two years post-surgery. Female athletes were more likely to fall into the lower resilience group, reinforcing why mental health support isn't optional in recovery — it's part of the protocol.
What this means practically: if you don't feel mentally ready to return, that's data. Share it with your care team. Psychological readiness is a legitimate return-to-sport criterion, not something to push through.
Know Your Options — Beyond the graft
Getting surgery is just the beginning. Recovery is where real strength is built — and it’s not just about doing exercises, it’s about understanding how your body heals and giving it the right tools at the right time.
HOW YOUR BODY ACTUALLY HEALS (AND WHY IT MATTERS)
Your body heals in 3 overlapping stages— and each one plays a role in how strong and safe your return to sport will be.
Inflammation (Days 1–3):
Swelling, heat, and pain show up fast. Your body’s cleaning the injury site and calling in immune cells to start repairs.
What I did: Rest, ice, compression, elevation. I moved gently without trying to overdo it.Repair Phase (Days 4 to ~6 weeks):
New tissue starts forming, but it’s weak and messy—like laying wet concrete. You’ll start light rehab here.
What I did: Focused on range of motion, quad activation, and reducing swelling.Remodeling Phase (6 weeks to months+):
That “wet concrete” gets shaped and strengthened. Your tissues learn how to handle force again.
What I did: Gradually loaded my body with strength work, balance drills, and sport-specific movement.
Key Reminder: Just because the swelling’s gone doesn’t mean you’re healed. Real tissue remodeling takes months, not weeks.
REHAB = YOUR NEW SPORT (FOR NOW)
Recovery isn’t just sets and reps. It’s mindset, consistency, and doing the basics every day.
Early wins = full extension, muscle activation, and pain-free movement.
Middle phase = balance, strength, mobility, and movement quality.
Late stage = return-to-sport testing, mental readiness, and high-level agility.
Athlete Tip: Track your progress with videos and journal entries — you’ll be shocked how far you’ve come in just a few months.
Note: Every injury—and every body—is different. If you have questions about your diagnosis, graft options, recovery timeline, or return-to-sport plan, talk openly with your surgeon. They’re there to help you understand what’s happening inside your body and what it means for your sport and future.
You deserve to feel informed and confident about your care. Don’t be afraid to ask.
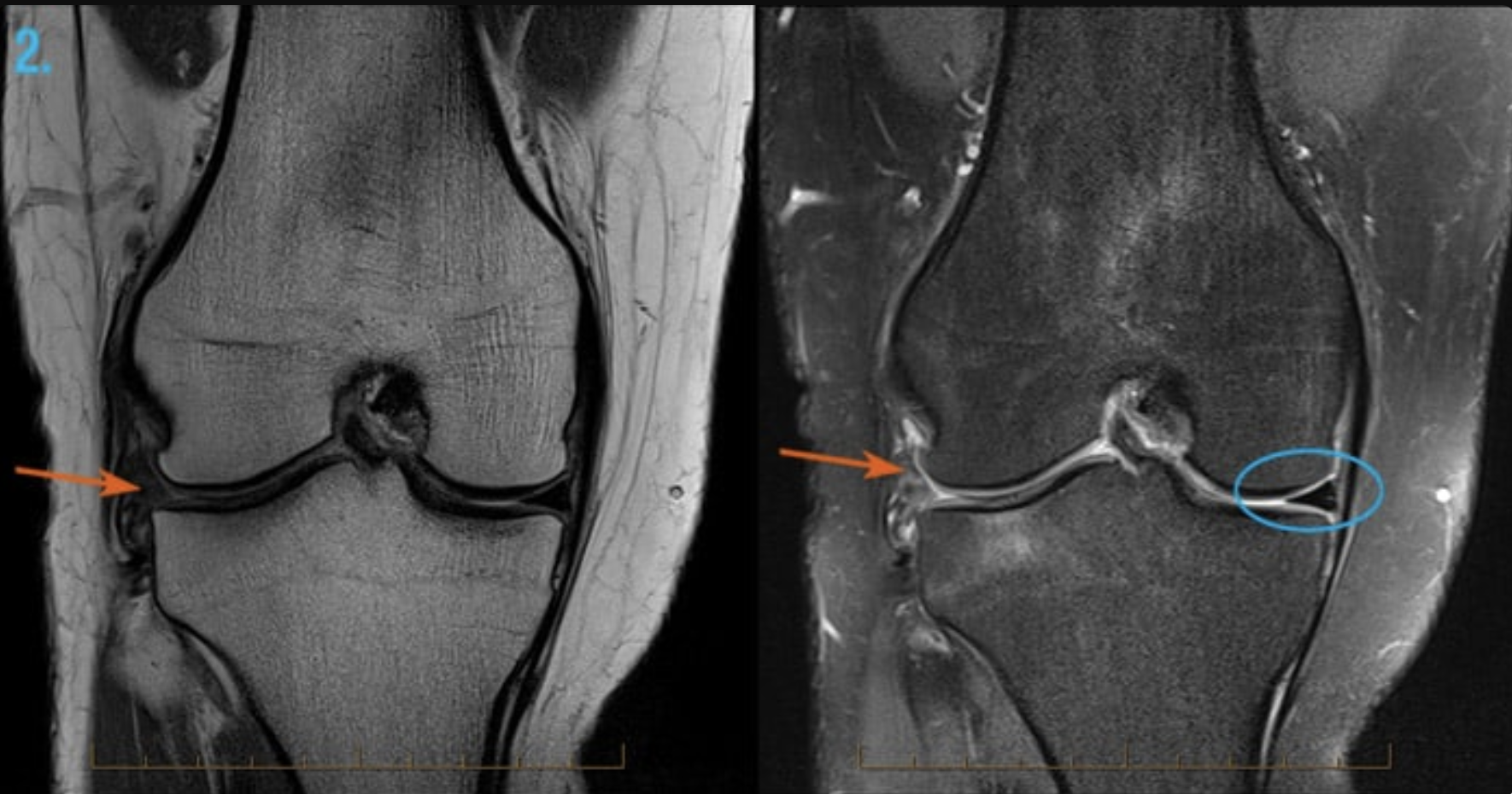
"HOW BLOOD FLOW COMES BACK AFTER ACL SURGERY”
After ACL surgery, it takes time for blood to return to the tendon and bone tunnel:
Blood flow reaches the femur side of the bone tunnel by 2 months—starting from arteries nearby.
Inside the new tendon graft itself, blood starts flowing again around 3 months.
On the tibia side, blood flow is slower to return but eventually improves — especially where arteries are closest.
Why it matters: Blood brings healing power. This slow return is one reason why full recovery takes 9+ months — even when you start to feel okay.
Read this Study — Re-vascularization to the bone tunnel wall after anterior cruciate ligament reconstruction may relate to the distance from the vessels →
Understanding the Healing Process — Diagrams
I made these diagrams to help you actually see what's happening inside your body
Note: The biological sequence shown in this diagram is based on research published in Skeletal Muscle Journal — Angiogenesis precedes myogenesis during regeneration following biopsy injury of skeletal muscle (2023) →. For a more accessible overview of the muscle healing process, visit Athletico Physical Therapy — Understanding the 3 Phases of Muscle Healing →
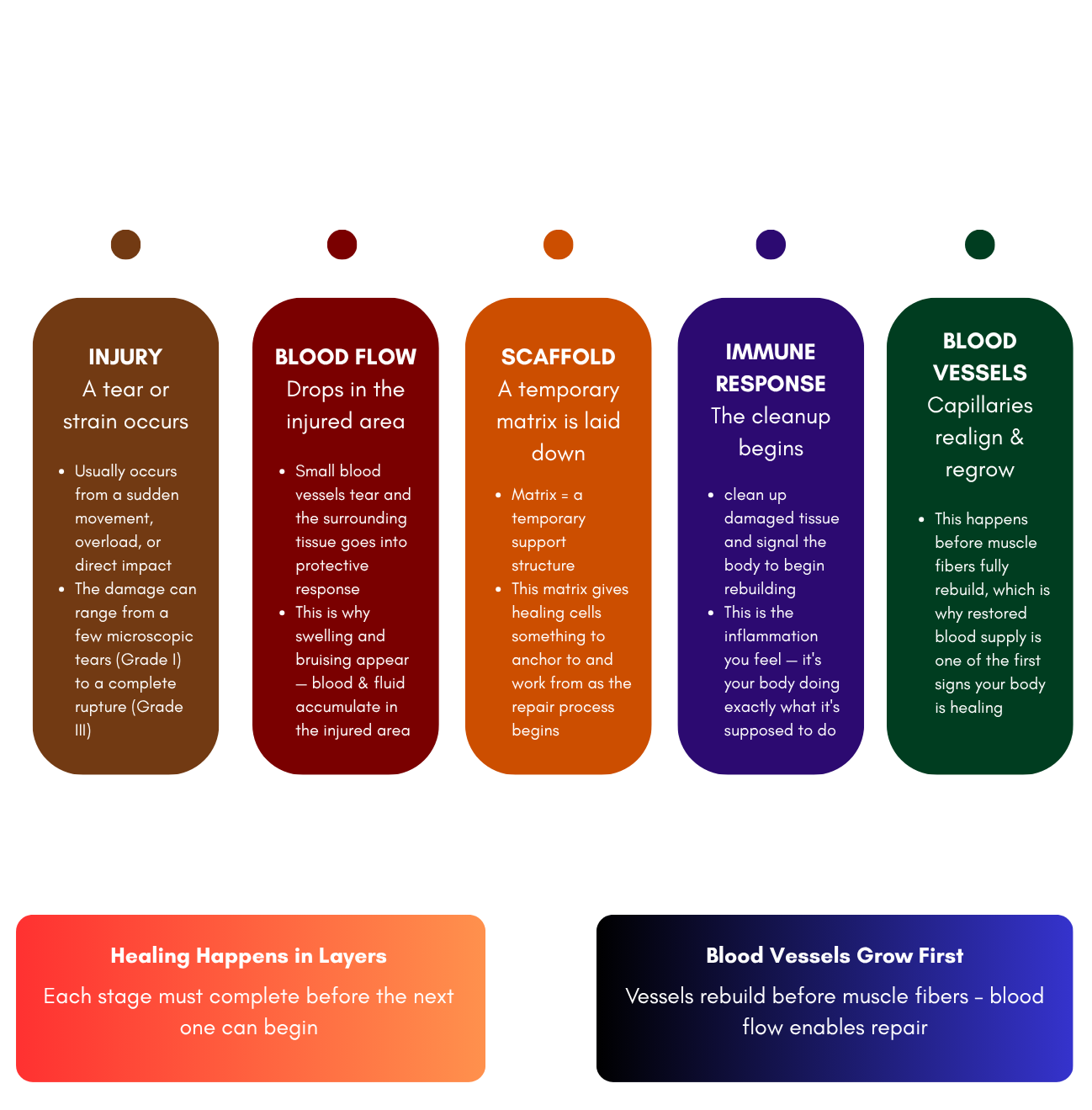
Key Insight: Your body doesn't skip steps. Even when a strain feels minor, this full sequence is happeninginside you. Returning too soon — before blood flow and repair are established — risks reinjury becausethe tissue hasn't finished rebuilding its foundation yet
Note: The three phases of tissue healing shown in this diagram are adapted from concepts presented in the NSCA's Essentials of Strength Training and Conditioning (4th ed.), Table 22.1 — Tissue Healing Phases →. This content was recreated in original format by RebuildYou for educational purposes.
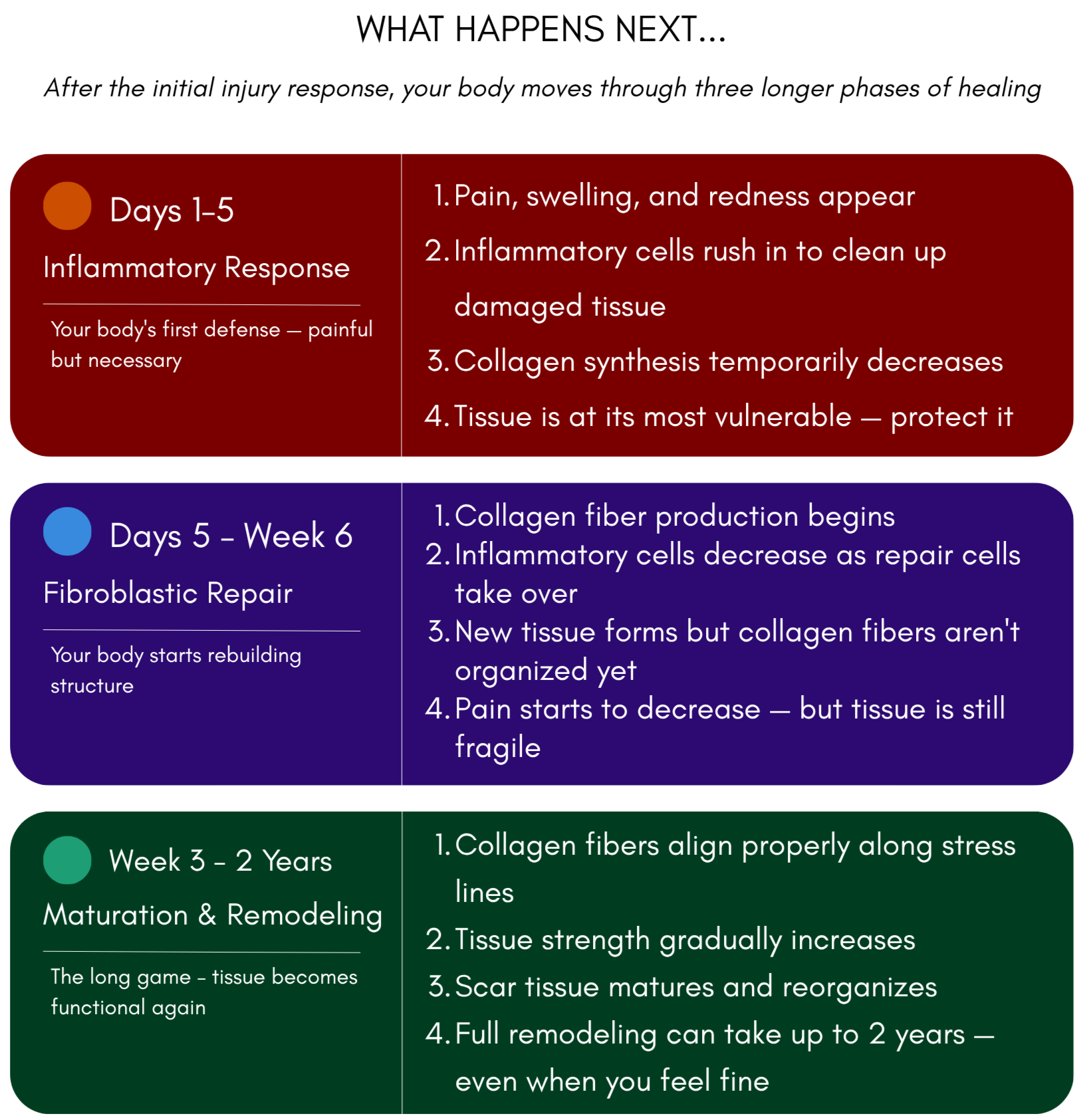
Why this matters: Feeling better doesn't mean you're healed. Pain disappears during the fibroblastic phase — but full tissue strength isn't restored until remodeling is complete. This is why returning too soon is one of the most common causes of reinjury.